Brain and Mind in Elite Sport: One Label, Two Very Different Evidence Bases

Prefer listening? Play the audio version:
This is the sixth piece in our series on the technologies actually changing elite sport in 2026. As ever, this is not a manual written from the touchline. It is a map of where the evidence is strong, where it is thin, and what a performance department should ask before letting any of it near a decision.
The cognitive layer of performance is usually sold as a single category: the brain as the last frontier, the place where the next competitive edge will be found. It is a tidy story, and it is misleading. What actually sits under that label is two enterprises moving at very different speeds and resting on very different foundations. One is the institutionalisation of athlete mental health, which over the past decade has crossed from taboo to standard infrastructure and rests on a serious and growing clinical evidence base. The other is performance neurotech, the headbands, stimulation devices and brain-training platforms sold to sharpen focus and reaction time, which rests on an evidence base that is real but small, heterogeneous, and routinely overstated in marketing. Treating them as one category flatters the weaker half by association with the stronger. This piece pulls them apart, because a performance director should approach them in almost opposite ways.
Mental health: the half that has genuinely matured
The shift in elite-sport mental health over the past decade has been generational, not incremental. A series of high-profile athletes, among them Kevin Love, DeMar DeRozan, Naomi Osaka and Simone Biles, chose to make their own struggles public, and in doing so changed what could be said openly in a locker room. That cultural change matters here only as context, and those disclosures belong to the athletes who made them. The point for a performance department is what came after: the cultural shift has been matched by structural change in how leagues and federations staff and fund mental health support.
The institutional markers are concrete. The major North American leagues have formalised league-level mental health requirements: the NBA requires teams to retain licensed mental health support and to identify psychiatric consultation, while the NFL-NFLPA behavioural-health agreement requires each club to retain a behavioural-health clinician available at the facility for a set minimum of hours per week. Together these frameworks formalise clinician access, emergency action planning, education and confidentiality procedures, although the exact requirements differ by league. Many federations and Olympic programmes have moved in the same direction, though the requirements are less uniform than in the closed North American leagues. The direction is unambiguous: mental health support has moved from optional to expected, sitting inside medical departments as a core clinical responsibility rather than a wellness extra.
The evidence underneath this shift is what makes it serious rather than performative. The International Olympic Committee’s consensus statement on mental health in elite athletes set out, for the first time at that level, that mental health symptoms and disorders are common in elite athletes, that they can impair performance, and that mental and physical health cannot be cleanly separated (Reardon et al., 2019). The prevalence data is sobering and dismantles the old assumption that fitness is protective. In a study of elite athletes applying for a national scholarship, lifetime prevalence of mental health problems was 51.7%, and 19.5% met clinical cut-offs for anxiety or depression at the time of survey (Åkesdotter et al., 2020). Those numbers are broadly in line with the general population, which is precisely the point: elite athletes are not exempt, and the institutions that pretended otherwise for decades were wrong.
One detail in that data deserves more weight than it usually gets, and it connects to a theme that recurs across this series. The sex differences are large. In the same study, women reported markedly higher rates than men, with 26.0% of female athletes reaching clinical cut-offs for anxiety or depression against 10.2% of men, and women were more than twice as likely to seek help (Åkesdotter et al., 2020). A mental health system designed around the average athlete is, in practice, designed around a presentation that differs by sex, and programmes that ignore that are leaving a known gap unaddressed.
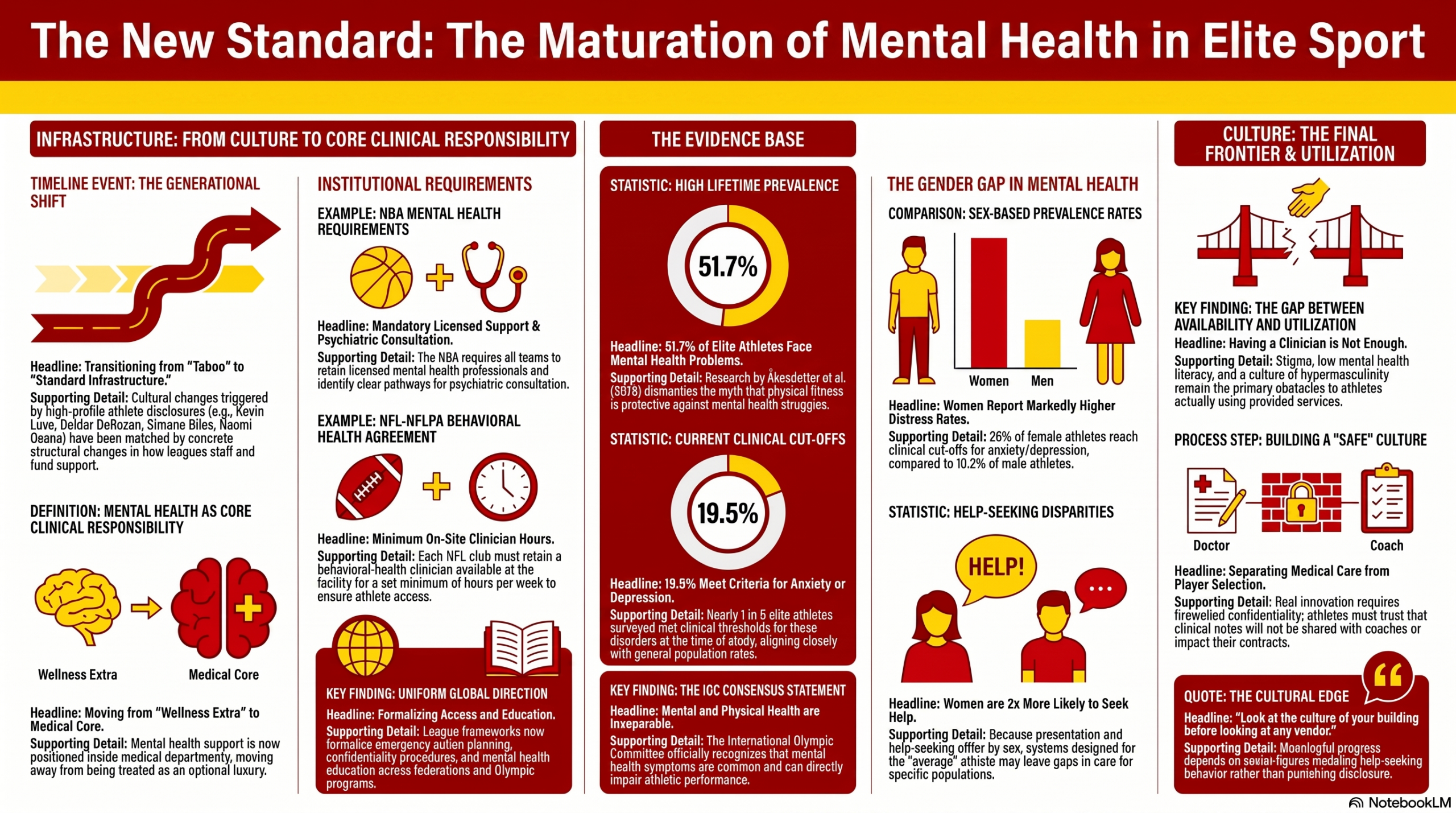
So the honest assessment of this half is that the infrastructure now exists and the evidence justifies it. The unfinished work is not whether to provide support but whether athletes actually use it. A systematic review of the barriers to elite athletes seeking mental health treatment identified stigma, low mental health literacy, negative past experiences with treatment, busy schedules and a culture of hypermasculinity as the recurring obstacles (Castaldelli-Maia et al., 2019). None of those is solved by hiring another clinician. The gap here is between availability and utilisation, and it is cultural rather than technological. A club can satisfy every staffing requirement and still have athletes who will not walk through the door, because the same competitive environment that produces the distress also punishes the disclosure of it. That is the real frontier in this half of the category, and no device closes it.
It also reframes what good looks like. In the mental health half, the meaningful innovation is not a product at all. It is the slow work of changing a culture so that the support already in place gets used: confidentiality that athletes actually trust, a separation between the medical and the selection conversation that is real and not nominal, and senior figures who model help-seeking rather than punishing it. A performance director looking for an edge here should look at the culture of their own building before they look at any vendor.
There is also a governance question that the rush to staff up has tended to skip, and it is sharper for mental health than for almost any other kind of athlete data. Psychological information is intimate, it sits inside an employment relationship, and the same record that supports a duty of care can, in the wrong hands, inform a selection or contract decision. An athlete who suspects that what they tell a club psychologist might travel to a coach has a rational reason not to talk. So the credibility of the whole system rests on a boundary that has to be real and not nominal: who can see clinical notes, how they are stored, what is firewalled from the performance and recruitment side, and whether an athlete can decline to share without it counting against them. A mental health programme that has not answered those questions in writing is not yet the asset its org chart claims.
Neurotech: real effects, smaller than the marketing, sold with more confidence than the data
The other half sits in an entirely different evidence position, and it is the half a performance director should approach with the scepticism this series applies to any category selling certainty ahead of proof. Brain-training apps, EEG-based focus trainers and transcranial stimulation devices have proliferated, typically promising substantial gains in reaction time, decision-making and competitive performance. The published literature supports a far more measured conclusion: the effects are real in places, but small, conditional, and concentrated in exactly the applications the marketing tends not to lead with.
Transcranial direct current stimulation is the most studied case and the most instructive. The most rigorous synthesis, a meta-analysis of 43 controlled trials, found that anodal stimulation of the motor cortex produced a small favourable effect on physical performance, a Hedges’ g of 0.29, with large heterogeneity and significant moderation by exercise type, training status and whether commercial or research-grade equipment was used (Winker et al., 2024). A small effect is not no effect, and for endurance tasks, where the perception of effort and central fatigue are limiting factors, the signal is most defensible. But two things should give a buyer pause. The heterogeneity is large enough that the prediction interval crosses zero, meaning some applications show no benefit or harm. And the effect is concentrated in physical, not cognitive, outcomes. A separate systematic review looking specifically at national- and international-level athletes found a single session improved strength or endurance in most studies but sport-specific tasks in fewer than half, with the high-level athlete evidence too heterogeneous to pool (Yu et al., 2024).
That second point is the one the marketing inverts, and it is the single most useful thing a buyer can know about this category. Neurotech is sold overwhelmingly on cognitive promises, sharper focus, faster decisions, better reaction time. Yet across the meta-analytic literature, the detectable effects of stimulation cluster in physical domains such as strength and endurance, while the aggregate effect on cognitive performance tends to come out smaller and less consistent. So the strongest evidence is for a physical effect, and the headline cognitive claims that actually sell the devices are the least supported part of the literature. A category that leads with its weakest evidence is telling you something about itself.
The commercial layer compounds the problem. The direct-to-consumer devices an athlete is most likely to encounter are not the research-grade equipment most studies used, and the gap between the two introduces variability the literature has barely addressed. For an elite team, the only defensible posture is experimental: a tool worth piloting for a specific, measured use case, most plausibly an endurance application, with a clear endpoint and an honest comparison, and never a generally validated performance enhancer deployed on the strength of a vendor’s reaction-time claim. The same applies to commercial EEG focus and neurofeedback platforms, where a systematic review of randomised trials found genuine potential but a field held back by non-standardised methods and inconsistent choices about which EEG signals to target (Cheng et al., 2024).
There is a further wrinkle that the category rarely raises about itself. Because some of these effects are real, however small, brain stimulation has already acquired a nickname in the ethics literature, neurodoping, and with it a question sport has not resolved: whether techniques such as tDCS should sit on the prohibited list at all, a question the World Anti-Doping Agency has had under active discussion (Petersen, 2021). If a device reliably improved performance, would it be permitted? The current effects are too small and too inconsistent for that to be a live regulatory issue, which is convenient for everyone, but it exposes the honesty problem at the heart of the marketing. A vendor cannot simultaneously claim that a device produces a meaningful competitive edge and that it raises no integrity question at all. Either the effect is large enough to matter, in which case sport will eventually have to rule on it, or it is small enough to be ignored by regulators, in which case it is probably too small to justify the purchase. The marketing tends to want it both ways.
Where the two halves actually touch
There is one genuine point of contact, and it is worth naming because it is the most defensible reason to keep the two halves in the same conversation at all. Virtual-reality tools, covered more fully in the immersive-training piece later in this series, sit across both. On the performance side, VR for decision-making and tactical recognition has one of the more plausible evidence bases in this neurotech-adjacent space, with a scoping review finding it a promising tool for assessing and training decision-making in team sports, though transfer to actual competition remains the key unresolved test (Jia et al., 2024). On the clinical side, VR-based exposure and anxiety-management techniques have an established evidence base outside sport and are being adapted for competitive anxiety and return-to-play after injury. That intersection, cognitive training that is also psychological support, is small but real, and it is where the label brain and mind is least misleading.
The reason VR sits more comfortably than the rest of the neurotech half is instructive. Its strongest applications do not claim to change the brain directly. They change what the athlete practises: more repetitions of a decision, a defence, a serve return, under controlled and repeatable conditions, with the difficulty and the scenario tuned to the individual. That is closer to a sophisticated training method than to a neurological intervention, and it is judged by the same standard any training method is, whether the skill transfers to competition. Framed that way, the burden of proof is clear, and the better study designs are beginning to meet it. The lesson for the rest of the category is that the tools with the best evidence are the ones making the most modest mechanistic claims. The devices promising to upgrade the brain itself are, so far, the ones with the least to show for it.
Approach the two halves in opposite ways
The practical conclusion is that one label should not produce one posture. The mental health half has earned institutional commitment: the evidence is serious, the prevalence is real, the sex differences are documented, and the remaining work is cultural, getting athletes to use support that already exists and is already justified. A performance department that treats mental health as core clinical infrastructure is following the evidence, not a trend.
The neurotech half has earned curiosity and caution, not commitment. The effects are real but small, concentrated in physical endurance rather than the cognitive domains the marketing emphasises, and muddied by the gap between research and commercial equipment. The right posture is the pilot, not the purchase order: a specific use case, a measured endpoint, an honest read of whether a small effect justifies the cost and the athlete’s time. So the position we would hold is this. Fund the mental health infrastructure as the clinical responsibility the evidence shows it to be, and judge every neurotech device against the question its marketing avoids: what exactly does it improve, by how much, in whom, and is that the thing you actually needed to change? The brain may well be the next frontier. That is a reason to hold its technologies to a higher evidential standard, not a lower one, because the frontier is exactly where confident claims outrun the data.
How this series is made, and how to read it: this is editorial analysis, not a practitioner’s memoir and not a systematic review. PERFORM’s pieces are researched and drafted with the assistance of AI tools, then reviewed, edited and fact-checked by our editorial team against primary sources, peer-reviewed literature, clearly labelled preprints, industry reports, league and company announcements, and practitioners’ own published work. Where the evidence is strong we say so; where it is limited we treat it as limited; where a claim comes from a vendor or corporate announcement we treat it as a hypothesis, not proof. The views here are our editorial position, drawn from the published record rather than first-hand experience inside an elite performance department. Where practitioners are named or quoted, those words are their own. Where we couldn’t verify a claim, we left it out. And where you have the hands-on experience we’re writing about, we’d rather hear from you than pretend to it.
References
https://doi.org/10.1136/bjsports-2019-100710
Cheng, M.-Y., Yu, C.-L., An, X., Wang, L., Tsai, C.-L., Qi, F., & Wang, K.-P. (2024). Evaluating EEG neurofeedback in sport psychology: A systematic review of RCT studies for insights into mechanisms and performance improvement. Frontiers in Psychology, 15, 1331997. https://doi.org/10.3389/fpsyg.2024.1331997
Jia, Y., Zhou, X., Yang, J., & Fu, Q. (2024). Animated VR and 360-degree VR to assess and train team sports decision-making: A scoping review. Frontiers in Psychology, 15, 1410132. https://doi.org/10.3389/fpsyg.2024.1410132
Petersen, T. S. (2021). Sport, neuro-doping and ethics. Neuroethics, 14(Suppl 2), 137–140. https://doi.org/10.1007/s12152-021-09461-z
Reardon, C. L., Hainline, B., Aron, C. M., Baron, D., Baum, A. L., Bindra, A., Budgett, R., Campriani, N., Castaldelli-Maia, J. M., Currie, A., Derevensky, J. L., Glick, I. D., Gorczynski, P., Gouttebarge, V., Grandner, M. A., Han, D. H., McDuff, D., Mountjoy, M., Polat, A., … Engebretsen, L. (2019). Mental health in elite athletes: International Olympic Committee consensus statement (2019). British Journal of Sports Medicine, 53(11), 667–699. https://doi.org/10.1136/bjsports-2019-100715
Winker, M., Hoffmann, S., Laborde, S., & Javelle, F. (2024). The acute effects of motor cortex transcranial direct current stimulation on athletic performance in healthy adults: A systematic review and meta-analysis. European Journal of Neuroscience, 60(5), 5086–5110. https://doi.org/10.1111/ejn.16488
Yu, Y., Zhang, X., Nitsche, M. A., Vicario, C. M., & Qi, F. (2024). Does a single session of transcranial direct current stimulation enhance both physical and psychological performance in national- or international-level athletes? A systematic review. Frontiers in Physiology, 15, 1365530. https://doi.org/10.3389/fphys.2024.1365530