FemTech in Elite Sport: Correcting a Data Gap Without Overcorrecting Into Hype

Prefer listening? Play the audio version:
This is the fifth piece in our series on the technologies actually changing elite sport in 2026. As ever, this is not a manual written from the touchline. It is a map of where the evidence is strong, where it is thin, and what a performance department should ask before letting any of it near a decision.
For most of the modern history of sports science, the athlete in the study was a man. Load models, recovery protocols, injury-risk frameworks and the validation cohorts behind most wearables were built largely on male physiology and then applied to women with little modification. That is a real and well-documented gap, and the correction now under way is overdue and welcome. But a correction can overshoot. The same momentum that is finally bringing female physiology into the design of performance technology is also producing a wave of marketing that claims more certainty than the science supports. This article tries to hold both truths at once: the data gap is real and worth closing, and the rush to close it commercially has outrun the evidence in places. Getting female-athlete technology right means taking the physiology more seriously and the product claims more sceptically, at the same time.
The gap is real, and the numbers are not subtle
Start with the part that is not in dispute. In a large study of physically active women recruited through Strava, researchers found that menstrual-cycle symptoms were widely associated with reduced ability to train and compete, and that the great majority of women had never discussed their cycle with a coach (Bruinvels et al., 2021). That sample was physically active women rather than an elite cohort, so it maps the broad problem space rather than proving the elite case on its own, and several authors were employees or consultants of a company that sells cycle-tracking software, a competing interest they declared. But the elite case is made directly elsewhere. In a cross-sectional study of 1,086 female athletes spanning sub-elite to top-elite level across 57 sports, 81% agreed that female-athlete health is treated as a taboo topic, only 11% had discussed it with their coach, and 53% rated their coach’s knowledge of it as poor or very poor (von Rosen et al., 2022). The gap is not a marketing invention. It is the documented default condition of women’s sport, at the elite level as much as below it.
So the structural correction is straightforward to justify. A 23-year-old swimmer arriving at a national programme in 2026 who encounters cycle-aware monitoring as standard practice is experiencing something her predecessor a decade ago almost certainly did not. That is a genuine institutional shift, and it does not depend on any single product being proven. It depends only on the prior situation having been indefensibly thin, which it was.
The science, read honestly rather than read to sell
The difficulty begins when the data gap becomes a marketing engine, because the underlying science is more cautious than the category’s loudest claims. Take the most common performance claim, that female athletes are dramatically weaker or stronger in particular cycle phases. The most rigorous synthesis, a network meta-analysis of 78 studies, concluded that exercise performance might be reduced by only a trivial amount in the early follicular phase compared with other phases, that between-study variation was large, and that the quality of evidence was low (McNulty et al., 2020). The authors’ own conclusion was that general guidelines cannot be formed and that a personalised approach is required. That is close to the opposite of the headline, sometimes seen in general-press coverage, that women perform dramatically worse at certain points in the cycle. The honest reading is that cycle phase has a real but small and highly individual effect on performance, which makes it a candidate for personalised monitoring, not for confident phase-based prescription.
There is a deeper reason the confident version of the claim does not hold, and it is methodological rather than physiological. The studies in this area define cycle phase, eumenorrhea, and even the start of the cycle in inconsistent ways, use small samples, and rarely confirm phase with hormonal measurement rather than calendar counting. That heterogeneity is not a footnote; it is the main reason meta-analyses keep landing on “low-quality evidence” and “personalise it” rather than a clean rule. A platform that converts calendar day into a training prescription is, in effect, treating a noisy and individually variable signal as if it were a precise one. The cycle is real, its effects are real, and the measurement of both is still too crude to support the certainty the dashboards imply.
The injury story is where calibration matters most, because it is both the most important claim and the most frequently distorted. It is true that female athletes tear their anterior cruciate ligament more often than men in comparable sports. But the gap is not uniform, and the single three-to-four-fold figure often quoted flattens that. In a meta-analysis of injury incidence by sex and sport classification, the difference was around three-fold in contact sports, but smaller in non-contact and limited-contact categories and in several cases not statistically significant (Montalvo et al., 2019). The direction is real. The magnitude depends heavily on the sport and the type of exposure.
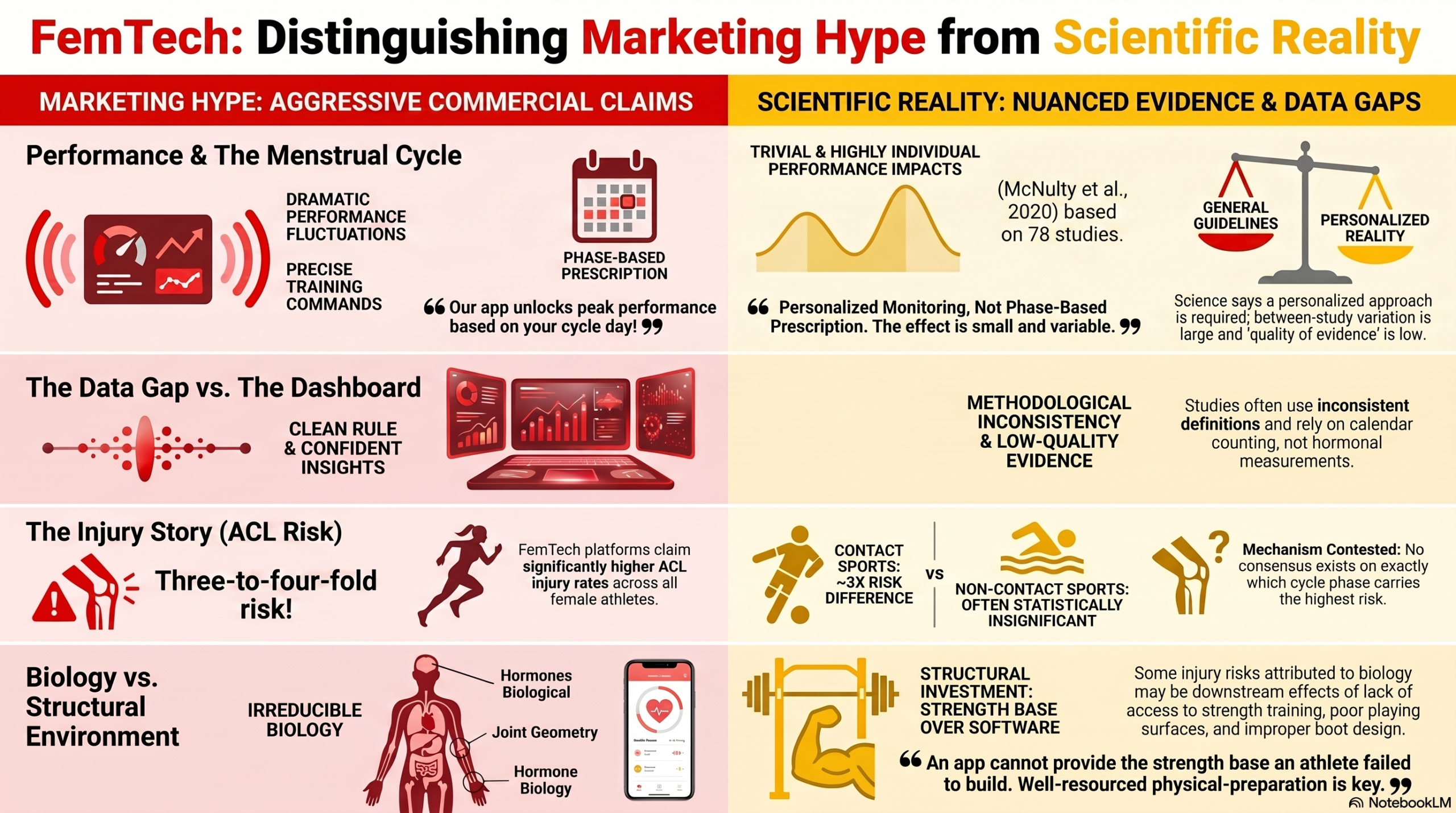
And the cause is genuinely contested, which the marketing tends to skip. The biological contributors are real, and none of this denies them: joint geometry, neuromuscular control patterns and hormonal effects on connective tissue are all plausibly involved. But a growing body of work argues that pinning the excess risk primarily on female biology is premature, because training history, access to strength and conditioning, playing surfaces, boot design and exposure patterns differ systematically between men’s and women’s sport. Some of what gets sold as irreducible biology may instead be downstream of the very under-investment this field is trying to correct. The relative weight of the two is not yet quantified, and that uncertainty is itself the argument for investment: the structural contributors are the ones a performance department can actually change. A cycle-tracking app cannot give an athlete the strength base she did not build at fifteen; a well-resourced, long-horizon physical-preparation programme can.
On the specific question of which cycle phase carries the highest injury risk, the literature does not agree with itself. Different reviews point to different phases, and the mechanistic surrogates, such as cycle-related changes in knee laxity, are real but vary in magnitude and do not translate cleanly into a known change in actual injury risk. The defensible position today is that hormonal fluctuation probably influences soft-tissue properties and therefore injury risk, but that nobody can yet tell a practitioner what to do differently on day 14 of a given athlete’s cycle with evidence behind it.
The products: a real category, marketed ahead of its evidence
Against that scientific backdrop sits a fast-growing commercial layer, and it deserves credit and scrutiny in equal measure. The most established player, the Galway company Orreco, with its FitrWoman athlete app and FitrCoach companion, has worked with elite female athletes for over two decades and frames its cycle-based guidance more cautiously than the category average, as risk-reducing and recovery-supporting rather than performance-transforming. That caution is to its credit and is the right posture. Other developments are structural: the women’s basketball league Unrivaled deployed an athlete-management platform across all its clubs from launch, which is notable because it builds women’s physiology in as a design assumption rather than retrofitting it. That is a genuinely interesting natural experiment in what a clean, women-first dataset produces.
The scrutiny is this. Both of those examples are evidence of commercial and infrastructural momentum, not evidence of improved female-athlete outcomes, and they should be read that way. The platform-reach claims come from company and sector material; the league-deployment claim comes from a vendor announcement, not an independent outcomes study. A cycle-tracking platform is, at its core, a structured data-collection and education tool, and on the current evidence that is exactly how it should be valued: as a way to close the conversation gap and to personalise monitoring, not as a validated performance-optimisation engine. When a vendor moves from “this helps athletes and staff track and discuss the cycle” to “this optimises performance around the cycle,” it has crossed from the defensible claim to the one the meta-analytic evidence does not yet support. That distinction is not pedantry. The defensible claim is genuinely valuable: if the documented reality is that most athletes never discuss their cycle with a coach and rate that coach’s knowledge as poor, then a tool that structures the conversation, normalises the logging of symptoms, and flags irregularities for referral is doing real work, precisely because the baseline was so low. A platform that gets an athlete and a clinician talking about a missed period, a pattern of heavy bleeding, or a run of poor-sleep, high-symptom days has earned its place. The overreach is only in the leap from there to a confident claim that the same app, by reading the calendar, can tell a coach how to programme training on a given day. The first is closing a communication and screening gap that the evidence says is real. The second is selling certainty the evidence says does not exist yet. The same market-signal-versus-evidence distinction we applied to the biomarker frontier in the wearables piece applies here: league adoption, athlete endorsement and venture funding are signs of momentum, not proof of effect.
The questions the category still skips
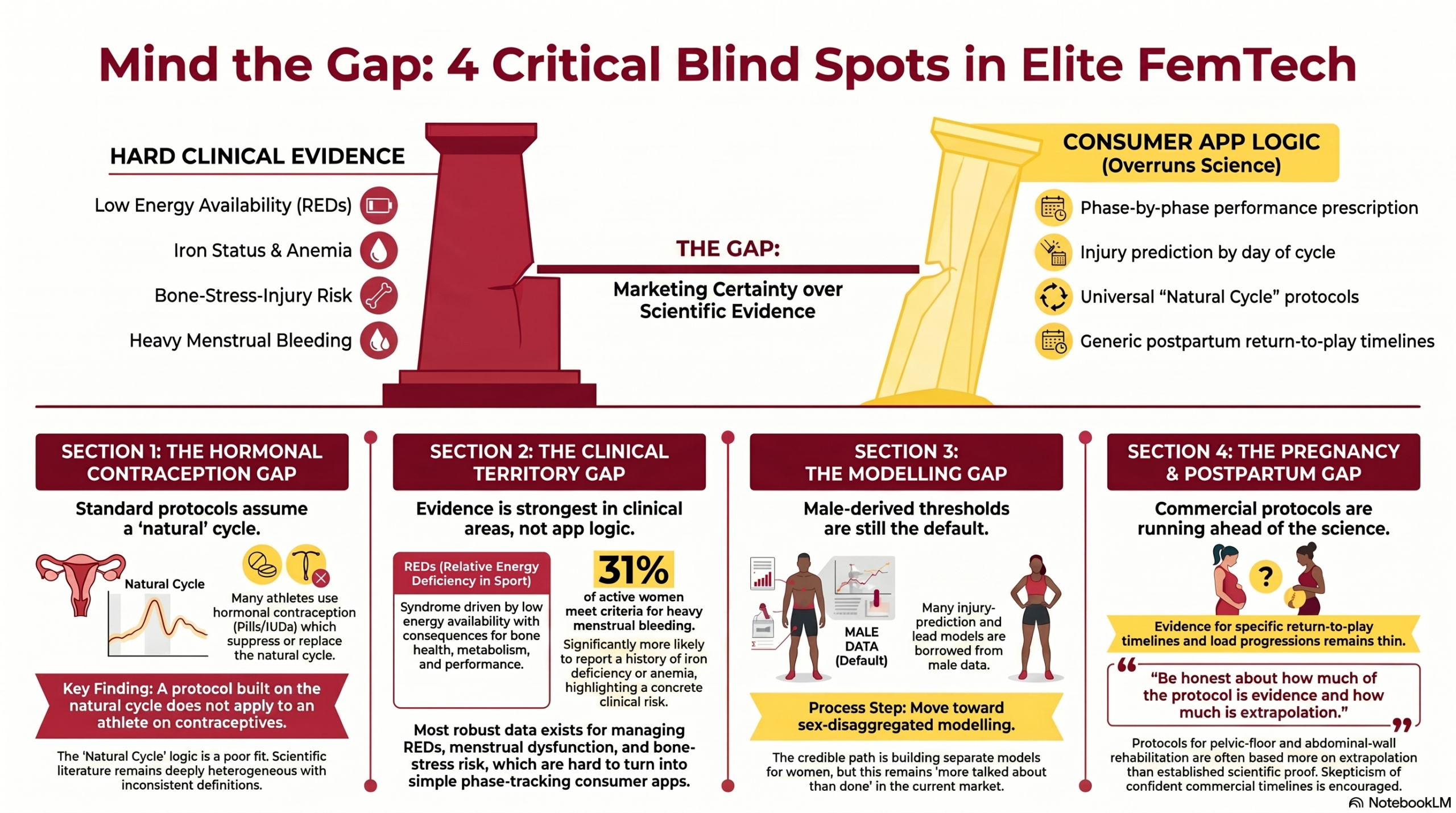
Three gaps are worth naming, because the vendors that endure will be the ones that address them rather than market around them. The first is hormonal contraception: a substantial share of elite female athletes use combined oral contraceptives or hormonal IUDs, which suppress or replace the natural cycle that cycle-tracking protocols assume. A scoping review of 96 studies on cycle phase, menstrual irregularities and contraceptive use in relation to injury found the literature large but deeply heterogeneous, with inconsistent definitions of cycle phase, irregularity and injury that make it hard to draw firm conclusions or compare studies (MacMillan et al., 2024). A protocol built on the natural cycle simply does not apply unchanged to an athlete on hormonal contraception, and few products say so clearly.
The second is the move from cycle-tracking into the harder clinical territory where the female-athlete conversation actually has the strongest evidence. Relative energy deficiency in sport is the clearest example: the 2023 International Olympic Committee consensus statement describes a syndrome, driven by low energy availability, with well-documented consequences across bone health, endocrine and metabolic function, haematology and performance, and notes that awareness of it remains low even among medical and performance staff (Mountjoy et al., 2023). Alongside it sit the female-athlete triad, bone-stress-injury risk, iron deficiency and heavy menstrual bleeding, areas with real, established clinical consequences for both performance and long-term health. The iron axis in particular is concrete rather than hypothetical: in a population screening study of recreationally active women, roughly 31% met the criteria for heavy menstrual bleeding, and those women were significantly more likely to report a history of iron deficiency or anaemia (Dugan et al., 2024). This is the uncomfortable truth the market tends to route around. The strongest evidence in female-athlete health is not in phase-based app logic; it is in detecting and managing low energy availability, menstrual dysfunction, bone-stress risk and iron-related problems, precisely the things that are harder to turn into a consumer app and easiest to miss when fatigue gets written off as training load. The third gap is sex-disaggregated modelling: where injury-prediction or load models are used, building and validating them separately for women rather than borrowing male-derived thresholds is the credible path, and it remains more talked about than done.
A fourth area sits slightly apart but belongs in the same honest accounting: pregnancy and postpartum return to elite performance. A series of high-profile athletes have made it a visible topic, and the cultural shift toward treating motherhood as compatible with an elite career is real and welcome. But the evidence base supporting specific return-to-play timelines, load progressions and pelvic-floor and abdominal-wall rehabilitation protocols is thinner than the public attention suggests, and it is an area where confident commercial protocols would be running well ahead of the science. The responsible posture is the same as elsewhere in this field: take the athlete population seriously, and be honest about how much of the protocol is evidence and how much is extrapolation.
Take the physiology seriously, take the certainty claims sceptically
The honest summary is that FemTech is correcting a real and indefensible gap, and that the correction is worth supporting on its own terms, independent of whether any specific product proves out. Closing the conversation gap, personalising monitoring, and designing systems around female physiology rather than as an afterthought are all genuine advances. But the science underneath does not yet support the confident, phase-by-phase performance prescriptions that the louder end of the market implies, the ACL risk gap is real but smaller and more context-dependent than the headlines, and its causes are partly structural rather than purely biological.
So the position we would hold is this. A performance director should treat female-athlete technology as a long-overdue correction to take seriously, and treat its specific performance claims with the same scepticism applied to any other category in this series. Buy the cycle platform to close the conversation gap and to personalise monitoring, which it can genuinely do. Do not buy it as a performance-optimisation engine, which the evidence does not yet support. Invest in the unglamorous, well-evidenced end, energy availability, iron status, bone health, strength programming, before the phase-based dashboard. If it reduces to a buying order, it is this: ask first what the product is actually for, education and communication, symptom logging, monitoring, or a performance claim, and be most sceptical of the last. Match it to the population, because a natural-cycle protocol does not transfer to an athlete on hormonal contraception. Be clear which evidence tier each claim sits on, from the well-supported (closing the conversation gap, screening for the clinical red flags) to the unsupported (phase-by-phase performance prescription, injury prediction by day of cycle). And screen the high-evidence clinical risks, low energy availability, menstrual dysfunction, bone-stress history and iron status, before buying any phase-tracking dashboard at all. And remember that the deepest correction this field can make is not a better app. It is treating female physiology as a default design assumption in everything from study cohorts to load models, so that the next generation of athletes never inherits the gap this one is still closing. The technology will help where it is honest about what it measures, but the correction will stick only if the institution changes underneath it.
How this series is made, and how to read it: this is editorial analysis, not a practitioner’s memoir and not a systematic review. PERFORM’s pieces are researched and drafted with the assistance of AI tools, then reviewed, edited and fact-checked by our editorial team against primary sources, peer-reviewed literature, clearly labelled preprints, industry reports, league and company announcements, and practitioners’ own published work. Where the evidence is strong we say so; where it is limited we treat it as limited; where a claim comes from a vendor or corporate announcement we treat it as a hypothesis, not proof. The views here are our editorial position, drawn from the published record rather than first-hand experience inside an elite performance department. Where practitioners are named or quoted, those words are their own. Where we couldn’t verify a claim, we left it out. And where you have the hands-on experience we’re writing about, we’d rather hear from you than pretend to it.
References
Bruinvels, G., Goldsmith, E., Blagrove, R., Simpkin, A., Lewis, N., Morton, K., Suppiah, A., Rogers, J. P., Ackerman, K. E., Newell, J., & Pedlar, C. (2021). Prevalence and frequency of menstrual cycle symptoms are associated with availability to train and compete: A study of 6,812 exercising women recruited using the Strava exercise app. British Journal of Sports Medicine, 55(8), 438–443. https://doi.org/10.1136/bjsports-2020-102792
Dugan, C., Peeling, P., Davies, A., MacLean, B., Simpson, A., Lim, J., & Richards, T. (2024). The relationship between menorrhagia, iron deficiency, and anaemia in recreationally active females: An exploratory population based screening study. Journal of Science and Medicine in Sport, 27(7), 437–450. https://doi.org/10.1016/j.jsams.2024.04.012
MacMillan, C., Olivier, B., Viljoen, C., Janse van Rensburg, D. C., & Sewry, N. (2024). The association between menstrual cycle phase, menstrual irregularities, contraceptive use and musculoskeletal injury among female athletes: A scoping review. Sports Medicine, 54, 2515–2530. https://doi.org/10.1007/s40279-024-02074-5
McNulty, K. L., Elliott-Sale, K. J., Dolan, E., Swinton, P. A., Ansdell, P., Goodall, S., Thomas, K., & Hicks, K. M. (2020). The effects of menstrual cycle phase on exercise performance in eumenorrheic women: A systematic review and meta-analysis. Sports Medicine, 50(10), 1813–1827. https://doi.org/10.1007/s40279-020-01319-3
Montalvo, A. M., Schneider, D. K., Webster, K. E., Yut, L., Galloway, M. T., Heidt, R. S., Kaeding, C. C., Kremchek, T. E., Magnussen, R. A., Parikh, S. N., Stanfield, D. T., Wall, E. J., & Myer, G. D. (2019). Anterior cruciate ligament injury risk in sport: A systematic review and meta-analysis of injury incidence by sex and sport classification. Journal of Athletic Training, 54(5), 472–482. https://doi.org/10.4085/1062-6050-407-16
Mountjoy, M., Ackerman, K. E., Bailey, D. M., Burke, L. M., Constantini, N., Hackney, A. C., Heikura, I. A., Melin, A., Pensgaard, A. M., Stellingwerff, T., Sundgot-Borgen, J. K., Torstveit, M. K., Jacobsen, A. U., Verhagen, E., Budgett, R., Engebretsen, L., & Erdener, U. (2023). 2023 International Olympic Committee’s (IOC) consensus statement on Relative Energy Deficiency in Sport (REDs). British Journal of Sports Medicine, 57(17), 1073–1097. https://doi.org/10.1136/bjsports-2023-106994
von Rosen, P., Ekenros, L., Solli, G. S., Sandbakk, Ø., Holmberg, H.-C., Lindén Hirschberg, A., & Fridén, C. (2022). Offered support and knowledge about the menstrual cycle in the athletic community: A cross-sectional study of 1086 female athletes. International Journal of Environmental Research and Public Health, 19(19), 11932. https://doi.org/10.3390/ijerph191911932